Gynecological Care
This includes yearly exams which vary depending on one’s age. I offer what is appropriate and cost effective for my patient’s yearly exams. Women who are 40 years or older should have a digital mammogram done yearly, as breast cancer risk increases with age. Pap tests should continue until age 70. Yearly exams can identify early and curable stages of endometrial, cervical, breast, and sometimes ovarian cancer.
A large part of my practice includes helping people with menstrual irregularities. In many cases, heavy bleeding or painful periods can be corrected without resulting to major surgery. Novasure ablation is a simple outpatient procedure that can correct abnormal bleeding without surgery. When needed, I can perform a hysterectomy to remove the uterus. Usually this is done when large fibroids are causing the problem and can often be done robotically. Abnormal Pap Smears are quite common ranging from atypical cells to severe dysplasia. I use ThinPrep Pap smears with HPV testing and perform thorough colposcopy when needed. Colposcopy is an office procedure where a microscope is used to look closely at the cervix to identify precancerous cells.
For those women having difficulty getting pregnant, I offer a compassionate approach to identifying and correcting the problem. For those who have completed their families, tubal ligation is available as an outpatient procedure. If one does not want to get pregnant, but does not desire permanent sterilization, other options such as IUDs, Nexplanon, Nuvaring, or birth control pills are available. I will help you to decide which is best for you.
Prenatal Care
I encourage patients to come in early when they discover that they are pregnant, but I accept patients at anytime during a pregnancy. An ultrasound is usually done on the first visit to confirm the due date. Typical appointments are every four weeks up to seven months, then every two weeks until your last month, when appointments are weekly. I perform all the standard and optional prenatal testing which is consistent among all doctors in Memphis, so I will not go into detail here. I do answer my own calls after hours as opposed to having a nurse on call. I deliver almost all of my own patients at either Baptist Women’s Memphis or Methodist Germantown.
US FDA Mercury Levels Found in Fish: This website lists mercury content in different fish. King Mackerel, Shark, Swordfish and Tilefish from the Gulf of Mexico are the highest and should not be eaten during pregnancy. Orange Roughy, most Tuna, Grouper, and Chilean Bass are moderately high in mercury, and should be avoided. Fresh tuna steaks and canned albacore tuna have higher levels of mercury than canned light tuna. Catfish, Crawfish, Salmon, Shrimp, Tilapia, and freshwater Trout are all low in mercury.
Preventative Care
This is a pathology diagram of a Pap smear from normal to more severe dysplasia, from left to right. As you can see, the cells get smaller and the depth of abnormality increases with worsening dysplasia (abnormal growth). CIN stands for cervical intraepithelial neoplasia. ‘Neo’ means new, ‘dys’ means abnormal
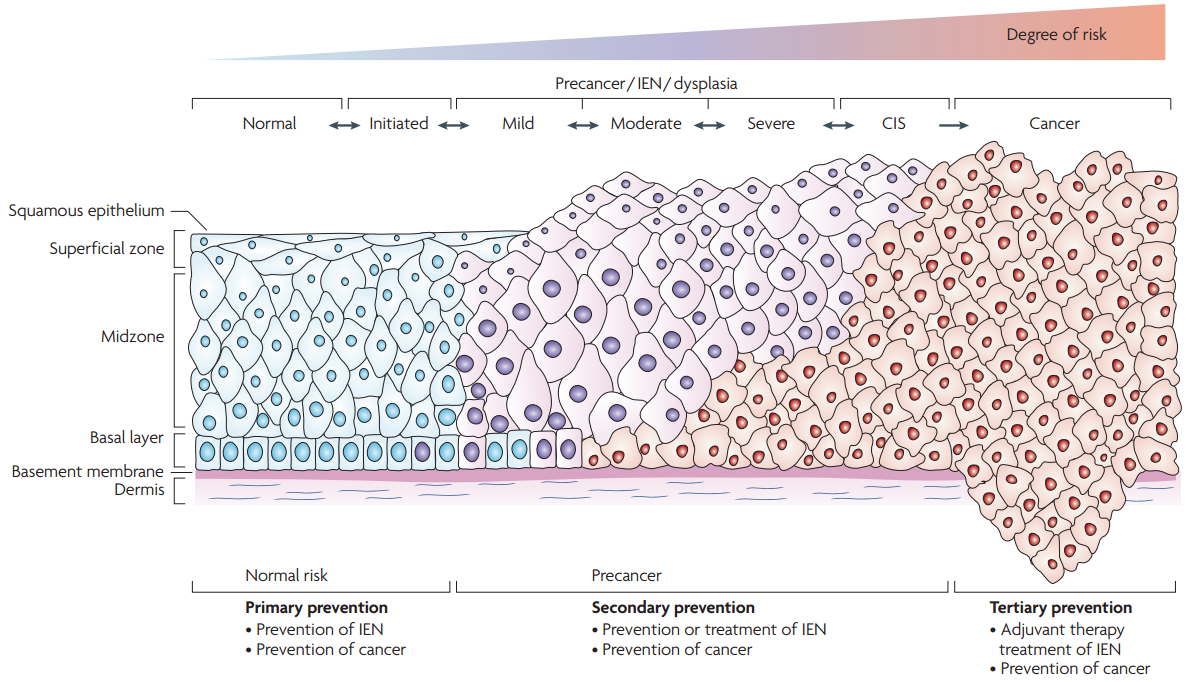
In Situ carcinoma is basically ‘cancer sitting there.’ At the bottom right, the abnormal cells have grown through the basement membrane or floor, such that they can now invade a woman’s body. This is true cancer. Everything else is precancerous. No one should get cervical cancer because it can be reduced with Gardisil and prevented with yearly Pap smears and follow up.
If you have an abnormal Pap test, you may be asked to return for a colposcopy. This is a simple office procedure in which your cervix is examined with a low power microscope called a colposcope. Acetic acid, or vinegar is applied to the cervix. This will cause any abnormalities to become white under the colposcope. A very small biopsy of any abnormal area is done. If the biopsy returns with dysplasia, the next step can be observation, cryotherapy, LEEP, or a cold knife cone (CKC), depending on your age and the severity of the dysplasia.
Something not on this diagram is a finding called ASCUS or atypical squamous cells of undetermined significance. Basically, this means that the pathologist who reviewed the Pap is saying that the cells do not look normal, but that they do not appear to be dysplastic or potentially cancer producing. Mild infections can cause this finding, or it may be that there are true concerning changes to the cervix that have not progressed enough to be identified as dysplastic. ASCUS is a very common finding. Until recently, most physicians would have a woman return in four to six months and repeat the Pap. With the addition of HPV testing, things have changed some. If I have a patient with an ASCUS Pap that also is positive for high risk HPV, I have the patient return for a colposcopy rather than waiting.
It is important to point out that testing positive for high risk HPV does not mean that you will get cancer of the cervix. We cannot say that HPV causes cervical cancer any more than we can say riding in a car causes a car accident, but you cannot get cancer of the cervix without having HPV, just like you cannot have a car accident unless you are in a car. In fact, it is estimated that as many as 80% of sexually active 18 year olds carry some form of HPV. I do not want you to think that I am downplaying the role of HPV in cervical cancer. Unfortunately, I have seen a lot of women with cervical cancer, and with rare exceptions, it was in women who did not get regular Pap tests or those who did not return for follow up on an abnormal Pap test. So please, get your yearly Pap done and tell me you hate it. I will understand.
Polycyctic Ovary Syndrome
The definition of polycystic ovarian syndrome, or PCOS, according to the NIH is an excess of androgen hormones and a condition of poor or no ovulation in cases in which other medical conditions have been excluded.
Most patients who see a gynecologist for PCOS, do so because they either cannot get pregnant, or they are having problems with their cycles. in addition, patients may complain about acne, facial hair, and difficulty losing weight. But there are many other concerns that should be addressed by the physician. First, it is important to know that PCOS increases one’s likelihood of having or developing heart disease, diabetes, and cancer of the uterus, and that women who become pregnant with PCOS have an increased risk of developing gestational diabetes, and blood pressure problems during their pregnancy. Women with PCOS whose pregnancies are induced with medications such as clomid are at a higher risk of ovarian hyper-stimulation, twins or more, and first trimester pregnancy losses.
Therefore, I believe that the best approach to PCOS is to start by treating the metabolic problems associated with the syndrome. By correcting these abnormalities first, cycle regularity, ovulation, and pregnancy will follow.
What causes PCOS?
Laboratory levels of luteinizing hormone (LH) and follicle stimulating hormone (FSH) have been used to diagnose PCOS. In addition, elevated levels of DHEA-S and testosterone can indicate hyperandrogenism or elevated male hormones. This is Stein-Leventhal Syndrome which has often been thought of as synonymous with PCOS. (Not everyone with PCOS fits the Stein-Leventhal characteristics). Patients should be tested for metabolic syndrome and insulin resistance, as these are two common conditions associated with PCOS. This begins with a check of your blood pressure and some weights and measurements. Your BMI or body mass index is calculated (weight in kilograms divided by height in meters squared). People with metabolic syndrome and/or PCOS generally have a BMI greater than 28. A waist to hip ratio may be done. People with PCOS gain weight more predominantly in their abdomens. A measurement greater than 0.72 is more common in PCOS and metabolic syndrome. Evidence of male pattern hair growth is often present, but not always. Metabolic syndrome is associated with elevated triglycerides, lower levels of the good cholesterol, HDL, elevated blood pressure and a high BMI. Insulin resistance is often associated with acanthosis nigricans, which is a velvety darkening of the skin, often seen on the neck and under the breasts. The best test for insulin resistance is debatable. I use a fasting insulin and glucose level. A 2-hour glucose challenge test, similar to the one used in pregnancy should be done. Other labs include an LH/FSH ratio, prolactin level, a thyroid panel, and a DHEA-S and testosterone level. Ultrasound can be performed to look for ovaries with multiple cysts.
Treatment
Treatment begins with reducing insulin levels and increasing SHBGs. Although medications can help, it takes more than just a prescription from your physician to treat PCOS. Proper nutrition and exercise are just as important in treating PCOS.
-
Medical Therapy:
Birth control pills are an effective treatment for women with PCOS who do not desire to conceive. Birth control pills with estrogen and progesterone have been shown to increase SHBGs, and to lower levels of LH and androgen or male hormone secretion by the ovaries. Birth control alone can often return one’s cycles back to normal. Birth control pills typically contain both estrogen and progesterone. Progesterone often has an unwanted side effect of increasing circulating androgens. Norethindrone, and ethynodiol have the lowest androgenicity while levonorgestrel has the highest androgenic activity, according to a leading authority on oral contraceptives, Dr. Richard Dickey, with whom I trained while in residency. Norethindrone acetate has greater androgen activity than just norethindrone. Drosperinone may actually have anti-androgenic properties, making it well suited for women with PCOS. Birth control pills vary not only in the type of progesterone, but also the amount, so some pills using a less androgenic progesterone may actually have more androgenic activity than a pill using a high androgenic progesterone in a lower dose. If you have PCOS and are taking Estrostep, Levlen, Alesse, or Ovral, then you are taking the wrong birth control. (Those pills I just listed are probably better for women with endometriosis). The addition of metformin can improve the action of insulin, and thus decrease the levels of insulin circulating in the blood. A reduction in insulin levels can result in an increase in SHBGs and consequently, a reduction in androgen levels. Metformin has also been shown to increase ovulation in women with PCOS.
-
Exercise:
Exercise makes insulin work better. Some researchers believe that PCOS might be due to a resistance of skeletal muscle to metabolize insulin. I could be that a low percentage of skeletal muscle reduces one’s ability to metabolize insulin. In other words, building up more muscle can metabolize more insulin, and thus reduce or reverse insulin resistance. I am not an exercise physiologist and am therefore reticent about recommending exercise programs. Instead, I am going to provide information on what I and some of my patients are doing. Anyone 35 or older who has not been exercising on a regular basis, should see a cardiologist for a treadmill or fitness test. I enjoy riding a bicycle, as I have done this since a child. I was never very good at team sports, but I rode my bike all over town, not realizing that it was exercise.
-
Weight Loss:
Consistent exercise will lead to weight loss, and the good news is that even as little as a 5% reduction in weight may cause a return to normal menstruation. 5% of 240 lbs would be just a 12 lb weight loss. A greater return to a normal weight and BMI can reverse many or all of the symptoms of PCOS without drug therapy.
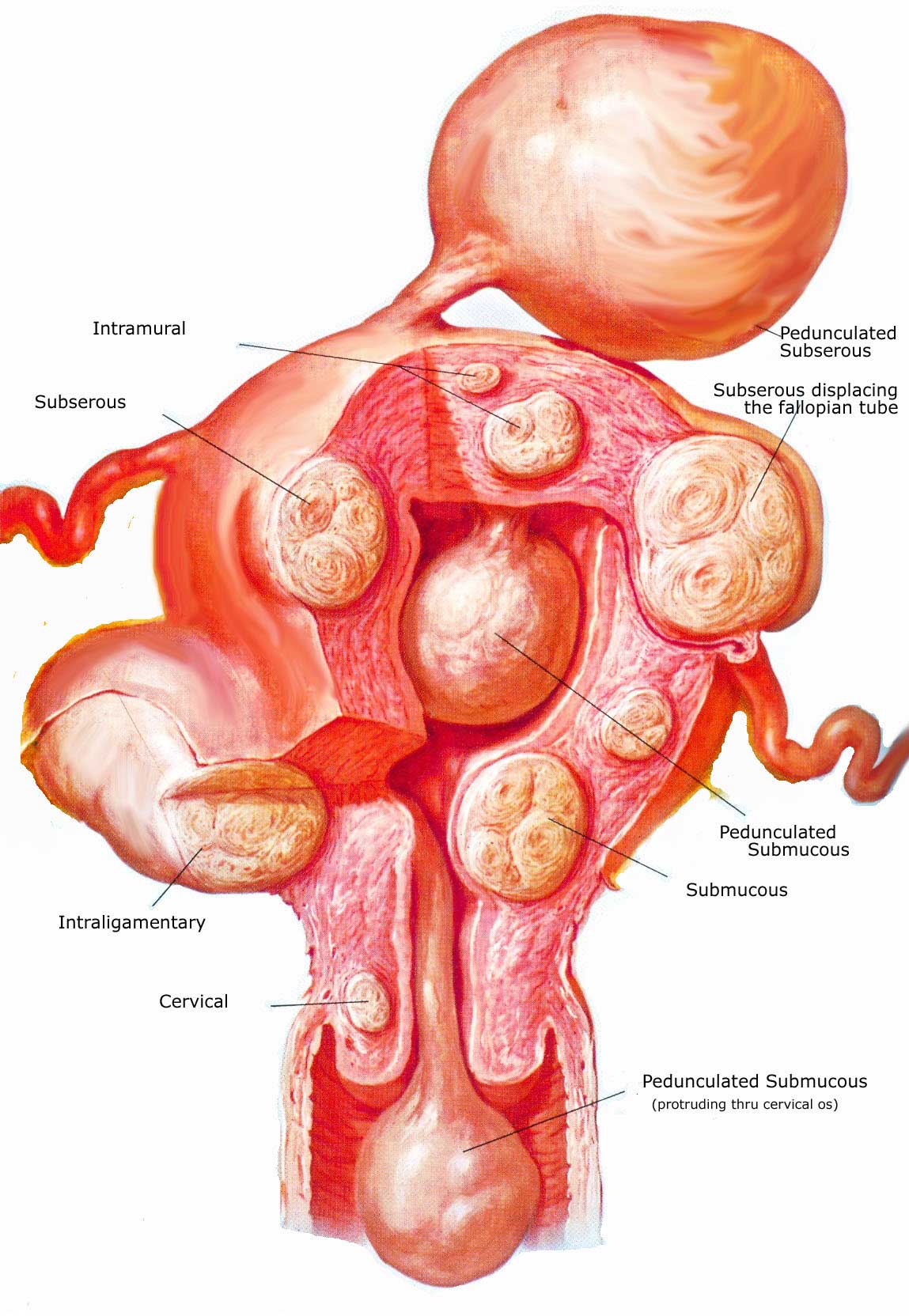
Uterine Fibroids (Leiomyomata)
Fibroids are so common that women with them are part of my practice every day. Fibroids are benign tumors of the uterus that usually do not appear, or at least do not present problems for women until after the age of 30. Rarely are they a cause of infertility. If you have been told you have fibroids, and you are not experiencing problems, such as heavy cycles, then chances are, there is no need to remove them. Any menstrual flow that lasts more than seven days is not normal. Passing clots, especially for more than the first two days of a cycle is abnormal. Heavy bleeding can lead to anemia which may indicate a need to remove the fibroids. Usually, fibroids do not cause pain, but sometimes fibroids can cause a uterus to push on nerves or the bladder or rectum, causing discomfort, constipation, urinary incontinence or frequency, or dyspareunia (painful sex).
Fibroids usually appear at the top of the uterus, known as the fundus, but they can occur anywhere on or near the uterus. Fibroids are described as being pedunculated, if they are attached to the uterus by a stalk. They can be subserosal if they are just below the outer surface of the uterus. Intramural fibroids, or fibroids in the muscular wall of the uterus, are the most common, and often do not cause problems, although they can get quite large. Occasionally a fibroid will penetrate or even grow into the cavity of the uterus. These are called submucosal and are the most likely to effect your bleeding, regardless of the size. Intracavitary fibroids are similar to pedunculated fibroids, but they are located on the inside of the uterus rather than the outside. These almost always cause bleeding abnormalities.
There are several different procedures to manage uterine fibroids, but the definitive treatment is hysterectomy. A hysterectomy is removal of the uterus via an abdominal incision, with the laparoscope, or through the vagina. It is important to know that your ovaries do not necessarily have to be removed with a hysterectomy. Ovaries provide you with your natural hormones, so if you can keep them, that is usually best.
Other less invasive procedures are possible depending on the location, size, and number of fibroids. With all other procedures other than hysterectomy, the woman may still have menstrual bleeding and the possibility that fibroids will return. Endometrial ablation involves destruction of the endometrium. The endometrium is the lining of the uterus that is shed each month. Ablation is an attractive option when the fibroids are small, as it does not require an incision or weeks off from work. There are four types of ablation. First is called the roller ball. In this procedure, a hysteroscope is used along with a small electrode that is used to burn the lining of the uterus. Compared to other procedures, it is time consuming, and I dare say that new physicians today probably are not trained in this method. I have done quite a few, but not in years.
Two other procedures burn the lining of the uterus. One is called balloon ablation and the other is Novasure. Balloon ablation is a technique in which a small balloon is inserted into the uterine cavity through the vagina and filled with water. The water is then heated to a temperature that will cause thermal destruction of the uterine lining. Another technique, that is faster, is Novasure. This procedure involves inserting a device into the uterine cavity, that then fans out to fill the cavity. This procedure is fast and effective if the fibroids are small. It may work better if the fibroid or fibroids are inside the cavity. Finally, there is Cryoablation. This involves freezing the lining of the uterus. Cryoablation is most easily done in the physician’s office compared to the other methods. I have stopped performing office Cryoablation as the results are not as satisfactory. All of these procedures only require a couple of days off work.
Ablation may completely prevent menstrual bleeding, but more often than not, a woman will still have cycles, although lighter, or she may have a return to menstruation months to years later. One other concern with ablation techniques is that it may hide a developing endometrial cancer. Endometrial cancer usually presents with abnormal or post-menopausal bleeding. Scarring of the uterine lining by ablation may prevent this warning sign from occurring.
A procedure performed by some radiologists called uterine artery embolization can be highly effective for women who have only one or two large fibroids. The radiologists locates the fibroids and passes a catheter through an artery supplying blood flow to a particular fibroid, then blocks the flow of blood to the fibroid causing the fibroid to deteriorate over time.
Myomectomy is a surgical procedure where the fibroids are removed, and the uterus is repaired. This can be done with a laparoscope, hysteroscope, or an abdominal incision depending on the location, size and number of fibroids. Myomectomy is the best option for women who still want to conceive.
There is one medication available that will shrink fibroids called leuprolide acetate. Lupron is a GnRH agonist that shuts down ovarian production of estrogen, essentially putting a woman into temporary menopause. Lupron can cause significant bone loss after a few months, and after the medication is stopped, the fibroids quickly return to their previous size. Lupron is a one month or three-month injection that costs several hundred dollars per injection. I sometimes will use Lupron for a short period of time to shrink really large fibroids, before performing a hysterectomy or myomectomy. Menopause in and of itself will cause a reduction in size and symptoms of fibroids.